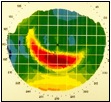
| Ken's Corner It’s all about centration Will proper treatment occur when Paragon CRT® lenses are decentered? Most often, the answer is, “NO.” During the initial fitting, we verify how the lens centers in an open eye situation and adjust the return zone depth (RZD) and the landing zone angle when necessary to fulfill the criteria for a “dispensable lens.” But treatment, of course, actually takes place in a closed eye environment. Topography verifies where treatment occurs in a closed eye. A perfectly centered lens in the open eye is, unfortunately, no guarantee that it will remain centered in the closed eye. Topography will show us where the treatment actually occurred during sleep and whether we’ll need to make an immediate parameter change. For those who do not yet have topography as an option, symptoms of flare and glare, distorted keratometric mires and induced astigmatism are telltale signs of decentration that may need immediate corrective action. It may be difficult to see a well centered trial lens in Asian eyes, and therefore the dependence on topographical results is paramount in those cases. Superior or lateral decentration is the most commonly reported centration issue. Proper treatment cannot occur with a lens that is decentered superiorly/laterally because the treatment zone is not positioned properly over the pupil and also because the treatment zone applanation is limited because of a “Z” axis tilt. —Hint: this is happening because there is complete fluorescein pooling, or no tangent touch (dark band) at 6:00 o’clock between the RZD and LZA. What is the best way to resolve superior decentration? Increase the sagittal depth of the lens, which can be done by:
Proceed with the above guidelines for achieving centration with a superiorly decentered lens. Note: There may be instances in which the limitations of the dispensing set do not allow a parameter change that will bring the lens to center. For instance: a larger diameter along with an LZA increase could be indicated, or a Paragon CRT® Dual Axis. Superior/lateral decentration occurs most often in the following instances:
Proper centration with Paragon CRT lenses is key. A slight loss of central applanation at dispensing may be necessarily acceptable, if it is the result of an increase in the RZD and/or LZA necessary to achieve initial centration. In this case, successful treatment will begin even if the optimum 4mm of central applanation is not present at dispensing. Subsequently, the sagittal depth may need to be reduced (a shallower RZD and/or a lesser LZA) to achieve full treatment. When all else fails - consider Paragon CRT® Dual Axis. Remember, centration is key to success! |

| Ken Kopp is Manager of Clinical and Professional Services at Paragon Vision Sciences. |
| | | | | |
| Questions? Contact: kkopp@paragonvision.com |
| Diagnostically, if the lens appears to decenter slightly superiorly, lift the upper lid. If the lens now drops to center, dispense it. If it does not drop to center, there is a good chance that the treatment would be superior with that lens if dispensed. |